
Vaping and Juuling: A youthful rite of passage or a camel’s nose through the tent flap?
Perhaps you saw the headline in the January 24 issue of The Charlotte News: “CVU responds to recent drug-related issues.” The story shed light on growing concerns among educators and policymakers about the appearance of vaping and juuling in schools. Are these part of some new dance or fashion craze? What does this have to do with drugs in our schools?
Even if you haven’t heard these terms, you may have seen people huddled outside doorways, puffing on small black tubes and exhaling much as they might if smoking cigarettes. If this is the case, you have seen people “vaping.” Vapers are inhaling a nicotine-laced vapor, or aerosol, produced by a battery-powered heating element immersed in a liquid. Hence the generic term: e-cigarette (see graphic). Juuls are simply one of the more popular brands of these devices, holding about 45 percent of the e-cigarette market. They look more like elongated thumb drives than cigarettes, and, just like a thumb drive, the device can be inserted in and recharged by a computer (see juulvapor.com/shop-juul/). They are not cheap. A starter set costs $45.
Nicotine, the critical ingredient in this vapor, is an extremely potent and highly addictive drug that is also an important component of tobacco smoke. It is the craving for nicotine and its effects that drives and reinforces smoking behavior. Nicotine definitely should be avoided by pregnant women since it is toxic to the fetus. Adults with chronic conditions may also be adversely affected. However, children and adolescents should avoid nicotine—not simply because of its addictive properties but because of its potential impact on brain development.
Harm reduction or gateway to nicotine addiction
It is important to recognize that e-cigarettes, like their tobacco-based counterparts, are nothing more than drug delivery devices. As such, one would expect that they would be highly regulated. Sadly this is not the case. Both federal and Vermont state law prohibit the sale of these “tobacco substitute” devices to persons under 18 years. However, the constituent parts of these devices: the contents of the liquid, the amount of nicotine produced, the heating element and the battery are not currently regulated by the Food and Drug Administration. In fact, President Trump’s newly appointed FDA commissioner, Dr. Scott Gottlieb, himself a former director of a major e-cigarette manufacturer, delayed the implementation until 2022 of stringent new marketing restrictions for these devices originally proposed under the Obama administration. In fairness, Commissioner Gottlieb has also explicitly stated the FDA’s desire to reduce the number of active smokers in the U.S.
While it is the addiction to nicotine that drives the cigarette market, it is the tar and other combustion products in cigarettes that kill people. It is precisely for this reason that e-cigarette advocates, as well as some well-recognized public health researchers, argue that there is an important role for e-cigarettes as part of a tobacco-control strategy. Although not yet proven, these devices may provide active smokers with a pathway to successful quitting by allowing them to gradually reduce their dependence on nicotine.
But public health advocates have pushed back against this “harm reduction” argument. First, they argue that many of these electronic devices use heat, liquid solutions and additives to produce aerosol vapors inhaled by the user. (These aerosols deliver nicotine to the lungs and ultimately to the blood stream.) None of these ingredients is currently regulated nor have their long-term health effects been studied. Second, they argue that, while these devices may be less risky for regular cigarette smokers, they may provide a gateway for young, never smokers, to experiment with and ultimately become addicted to nicotine.
A recent, totally unscientific, survey by this writer suggests that, among local high school students, as many as 25 percent of kids have been “one-time,” “casual” or “sometimes” users of these electronic devices. This contrasts with the CDC’s 2016 survey for the U.S. that reports a far lower percentage of school users: four percent in middle school and 11 percent in high school. Whatever the actual percentage of users in the school-age population, it is too high, as it is from these kids that big tobacco plans to recruit its next generation of cigarette smokers.
Lest you think this is an overreaction, consider the fact that an R.J Reynolds subsidiary owns VUSE, Altria (formerly Phillip Morris) MarkTen and British American Tobacco Vype, all popular e-cigarette brands. Phillip Morris is seeking FDA approval to market a new product called IQOS in the U.S. as a safer smoking device. Currently sold in over 30 countries world-wide, IQOS uses a battery-driven heating element to “heat but not burn” real tobacco, thus producing nicotine-infused vapor. The FDA has yet to rule on the IQOS claims.
How should schools respond?
So where does this leave school administrators and policymakers who have a legitimate and important interest in protecting and promoting the health of our kids? Should we view the use of these products and devices in schools as just another youthful rite of passage? Or should these devices be seen as part of a carefully orchestrated plan by the major tobacco companies to lure kids down a pathway leading ultimately to further dependence on their products? The history of big tobacco’s marketing successes in reaching kids is impressive—just think Joe Camel, among many others. To paraphrase Erika Sward of the American Lung Association: This is likely part of the end game for the tobacco industry, since we’re not talking about an industry that has demonstrated an interest in saving lives.
As parents, grandparents and concerned citizens we need to support schools’ efforts to discourage the further adoption of these behaviors. It is also important that we not transform e-cigarette devices into some kind of “forbidden fruit.” If we do, it will only increase the likelihood that kids will want to try them. But we do need to be clear about the real goals of the industry and the far-reaching effects of nicotine dependence. What’s most heartening is that the research shows clearly that if we can get our kids to the age of 21 or 22 without them becoming addicted to these products, then they most likely never will.
It took a generation to reduce the prevalence of smoking in this country. Surely we should do all we can to preserve that legacy.
Jim Hyde is associate professor emeritus at the Tufts University School of Medicine. He lives in Charlotte.
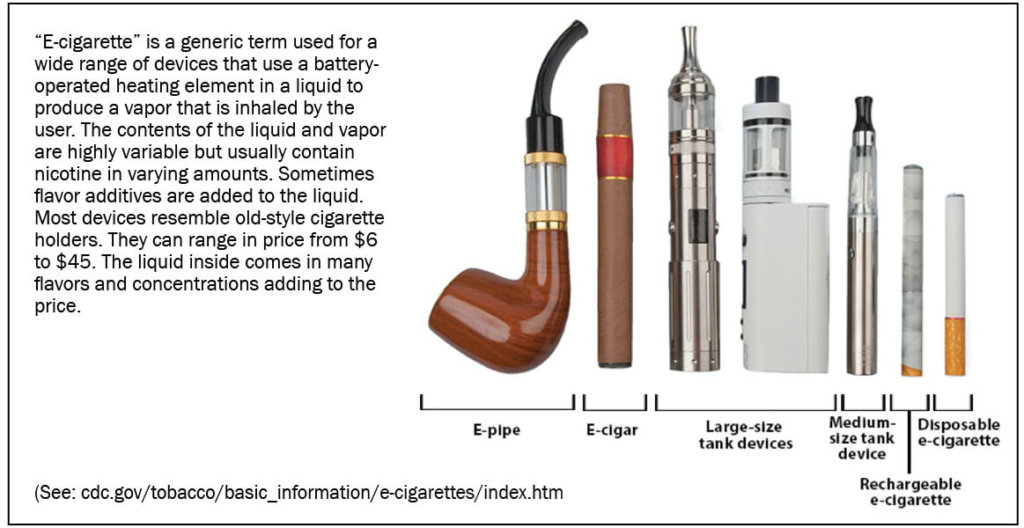
Sidebar: “E-cigarette” is a generic term used for a wide range of devices that use a battery-operated heating element in a liquid to produce a vapor that is inhaled by the user. The contents of the liquid and vapor are highly variable but usually contain nicotine in varying amounts. Sometimes flavor additives are added to the liquid. Most devices resemble old-style cigarette holders. They can range in price from $6 to $45. The liquid inside comes in many flavors and concentrations adding to the price. More information on the CDC website.